Central Airway Obstruction
^da8da2
General
- Most often arises as a complication of thoracic malignancies but a number of benign processes may also produce CAO including prolonged intubation
- CT imaging is valuable in this setting to detail the presence and extent of obstruction
- Flow-Volume loops are an excellent screening tool for CAO
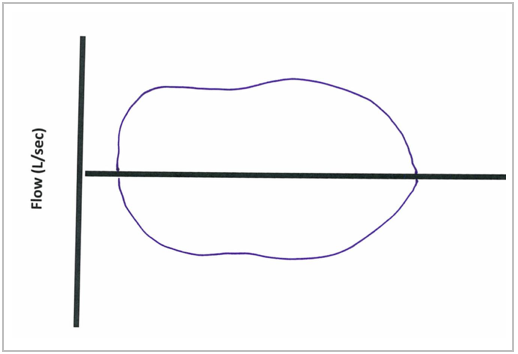
Fixed CAO
- Truncation of both inspiratory and expiratory flow limbs
- Etiology: Malignancies, post-intubation tracheal stenosis
- Post-intubation Tracheal Stenosis
- present at the level of the larynx due to direct trauma from ETT followed by scar formation or more commonly at the level of the ETT cuff (pressure effect of the cuff on the tracheal mucosa impairing perfusion → ischemic injury → scar formation)
- Due to this cuff pressure, those with prolonged intubation, you can tolerate a minimum leak to maintain the lowest possible pressure in the cuff
- Treatment -- balloon dilation, stunting, laser resection +/- mitomycin C and/or steroids to prevent regrowth of scar tissue → all done by bronch
- If bronch fails → surgery
Variable CAO
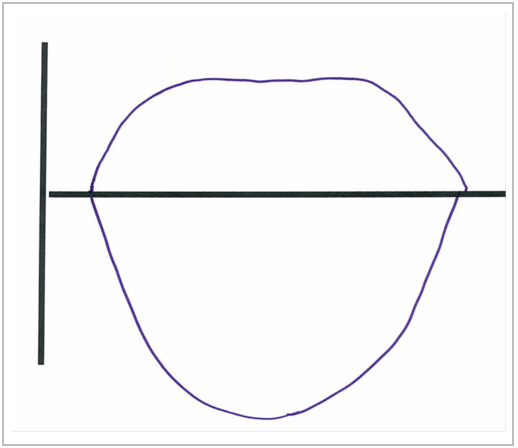
Intrathoracic Variable CAO
- Truncation of expiratory limb and preservation of inspiratory flow pattern
- Etiology: Tracheomalacia
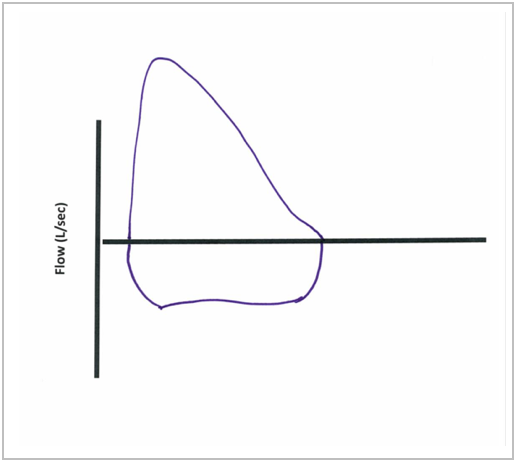
Extrathoracic Variable CAO
- Truncation of inspiratory limb and preservation of expiratory flow pattern
- Etiology: Tracheal crush injury in the neck